
Introduction To Policy
The Affordable Care Act (ACA) was enacted in March 2010, under President Obama, with the aim of expanding affordable healthcare coverage to millions of Americans. This is a federal law, and thus it required congressional support before eventually being signed by the President. According to the Department of Health and Human Services (HHS), the law has three primary goals:
- “Make affordable health insurance available to more people. The law provides consumers with subsidies (“premium tax credits”) that lower costs for households with incomes between 100% and 400% of the federal poverty level (FPL).
- Expand the Medicaid program to cover all adults with income below 138% of the FPL. Not all states have expanded their Medicaid programs.
- Support innovative medical care delivery methods designed to lower the costs of health care generally.”
The general theme here is about lowering the cost of healthcare, targeting lower-income individuals so that they can have better access to healthcare. Additionally, there are some notable regulations that the ACA added, such as prohibiting insurance companies from denying coverage or raising prices based on pre-existing conditions. This means that if the law works as intended, people would not be punished or disadvantaged in the healthcare insurance market for having health problems before getting coverage.
When originally enacted, the ACA also had an important provision called the “individual mandate”, which required all Americans to either get health insurance or pay a tax penalty. The main purpose of this provision was to expand the spending pool in health insurance, which forces otherwise healthy people to also chip in, thereby lowering the average cost of health insurance. Without the mandate, healthier individuals would be less likely to get health insurance, and thus, you would not be able to counterbalance the costly effect of dealing with “high-risk” individuals in the market. Another term for this is “risk-pooling”, balancing high-risk patients with low-risk patients so that healthcare costs are not too high for those who need care.
Further Context: Basis for Reform, Stakeholders & Interest Groups
Before the passage of the ACA, which is often called “Obamacare”, the U.S. healthcare system was quite fragmented, with approximately 45 million Americans uninsured. President Obama initially supported a public option, a policy that would provide a government-funded healthcare system to compete with the private market; however, due to opposition within his party, especially from more moderate Democrats, Obama had to settle for a more moderate option, which became the ACA.
Much of the support for the ACA came from organizations like the American Medical Association, American Hospital Association, and PhRMA, which the Obama administration sought out. Other organizations, including Families USA, an organization that claims to be a voice for healthcare consumers, also lent support for the ACA, including the controversial individual mandate. However, there is the case that the policy punishes small businesses, as argued by the U.S. Chamber of Commerce; their argument is that the ACA’s individual mandate imposes a cost on businesses with 50 employees or more, because of the requirement for these businesses to subsidize the healthcare coverage of employees. This is a fair criticism, despite it coming from a group with its own interests at stake in the case. If we are forcing employers to pay part of the cost of health insurance, and also pushing more people to get health insurance, does this not harm businesses that cross the 50-employee threshold? Arguments like these have led to skepticism of the ACA, and it is why it has been controversial even post-enactment, unlike Medicare, which became far more popular post-passage.
Another reason for the partisan divide, as stated by Oberlander, was that the ACA was targeted toward the “undeserving” poor in the conventional conception. This means that because the policy was not a universal program like Social Security or a policy that targeted children or elderly people – groups who have conventionally been targeted with more generous government transfers – it was harder to garner popular support for the ACA.
In general, we see tension here. The ACA aimed to balance voters’ concerns about the lack of affordable healthcare coverage with the concern that overhauling the system would disrupt the private market. President Obama and the Democratic majority thus had to walk a fine line between catering to consumers and to businesses, the latter of whom may not take kindly to government interventions in the market. As for ascertaining the “unseen” players in shaping the ACA, the likely answer includes the business interests the administration had to court, including health insurance companies that may benefit from a larger healthcare insurance pool. While the public opposition is often framed in the context of Republicans voting against the legislation, the business interests the Obama administration had to court were key players that were not as publicly displayed.
The Unseen: The Secondary Goal of The ACA
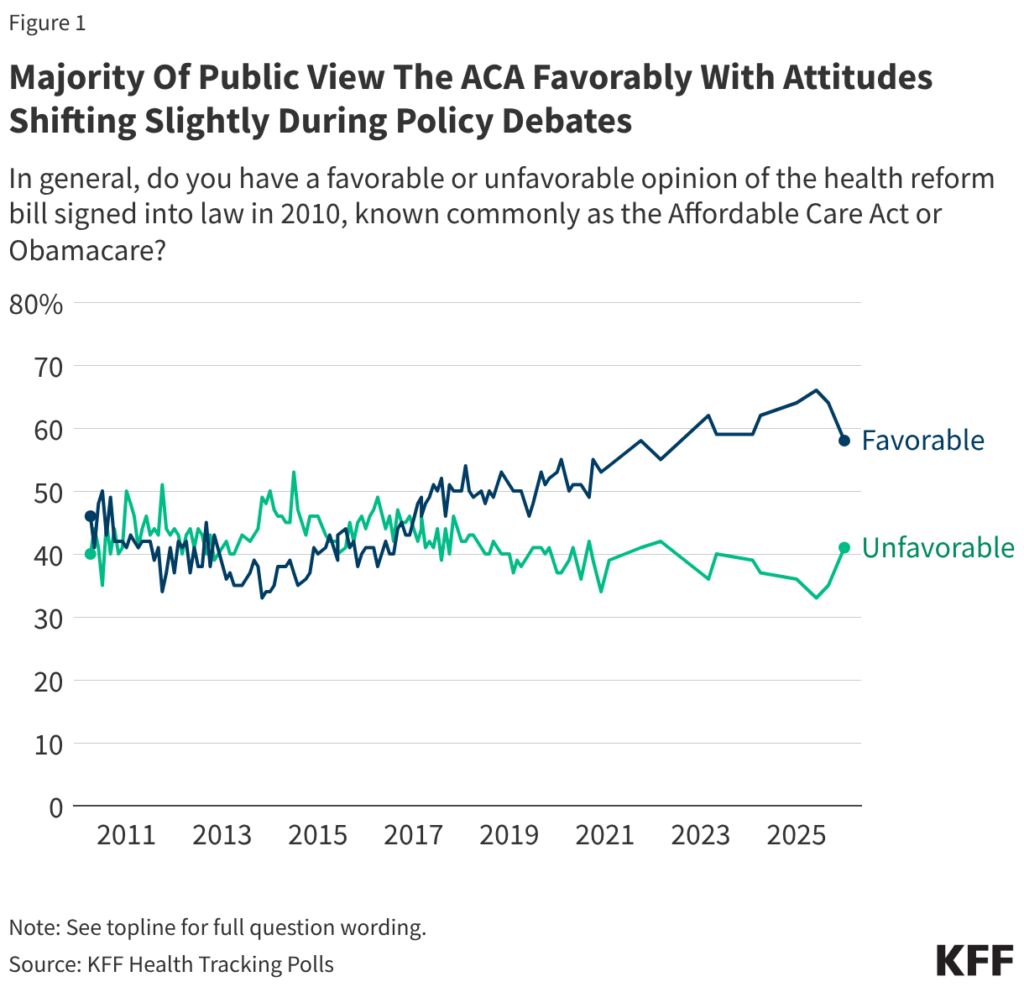
Much of the effect of the ACA can be framed in terms of its direct policy goals, which include the expansion of healthcare insurance, the implementation of new regulations and standards, and investments that make healthcare more affordable for certain income groups. However, one secondary goal could be that the ACA has set the groundwork for something bigger. Since the Trump administration failed to repeal the ACA in his first term and has not yet proposed doing so in his second, it seems like the ACA is here to stay, despite successful efforts to hamper the policy. Public opinion tracks this durability. After the failed 2017 repeal effort, the law’s favorability flipped net-positive and has stayed there since, reaching 58% favorable in January 2026, according to KFF polling.
Considering Obama’s original position was closer to a public option, a conceivable goal of establishing the ACA as a framework is to push the ball forward and build momentum for an eventual policy that inches closer and closer toward a public option. President Obama, by choosing this route, may have also instilled his legacy as someone who was capable of doing this – but this is where the subsequent administrations failed to do something of a similar vein. The use of the term “Obamacare” was effective branding by Republicans to muddy support for the reform on partisan terms. But President Obama eventually embraced it, and it has now become a part of his legacy.
Unintended Consequences: Hindsight and Alternative Framing
It is easy to critique the choices of policymakers in hindsight, but we must note that we are tackling an immensely complicated healthcare system with many significant players that are resistant to sweeping changes. That being said, we should analyze some areas where the ACA may have fallen short, both as a policy and political tool.
As a piece of policy, the weakness of the ACA is that it still does not provide universal coverage, and thus, the benefits are unclear. Oberlander’s report describes this more aptly when he states that Medicare and Social Security had a more “coherent programmatic identity”. This is to say, unlike those landmark policies, the ACA had bits and pieces of different policies seemingly muddled together in a complicated landscape; thus, it was difficult to properly simplify. As a policy tool, the ACA is successful, but because of its many moving parts, the politics surrounding it were difficult to sell to average voters. Complicated policies with such moving parts are also easier to undermine, considering the reliance on state implementation. As Oberlander notes, Republican legislatures ensured they could use this weakness to make the ACA harder to enforce. I also would like to note that Trump being able to gut the ACA’s individual mandate is another example of how a policy can be weakened over time, given that the individual mandate is a necessary prong to bring enough health insurers into the market to drive down costs.
The other potential unintended consequence of the ACA is that this is now a framework Democrats have to work with, for better or worse. Repealing the ACA wholesale, to put forth Medicare for All, or a public option, may be unpopular; it may seem disloyal to part of the Democratic establishment that wishes to protect the legacy of Obamacare. This tension is something you can see in the 2016 Democratic Primary debates between Hillary Clinton and Bernie Sanders. It may well be why the Biden administration failed to create something new, beyond that existing framework. Yet, depending on who you ask, this could well be an intended consequence of the policy design.
In hindsight, the Obama administration should have started with an understanding that the Republicans would not vote for his proposal, despite Obama’s efforts to compromise on key provisions. Instead, the primary goal would be to court only Democratic and left-aligned independents in both chambers of Congress. Then, working with that framework, his aim would be to pass something closer to a public option, with a universal application, so that the selling point of the policy is more coherent.
Of course, if moderate Democrats do not lend support, and he cannot pass the policy through Budget Reconciliation to avoid the filibuster, then he should have worked around that by trying to pass a version of the ACA that is at least more generous. As stated by Oberlander, “President Obama asked Congress not to exceed a total of $900 billion in spending on the ACA over its first decade, which led Democratic lawmakers to reduce the generosity of insurance subsidies and coverage”. This is a “self-inflicted” wound, where Obama weakened his negotiating position without needing to. Of course, one can argue that his reason was due to pressure from business interests and stakeholders he was trying to court, but we have no evidence to suggest that this move was necessary. Therefore, instead, President Obama should have signaled to Democrats that they can spend much more, and whatever is necessary to ensure the proper application of the enacted law. More generous subsidies can also provide more immediate benefits, which the Democrats could have run on during elections preceding the passage of the ACA. However, as already noted, passing a public option, if possible, would have been the more effective solution so that the benefits of the program can be explained to voters easily.
Finally, instead of a punitive application of the individual mandate, perhaps a more popular design is one that uses strong, positive tax incentives for people to get health insurance; while it may not be as powerful as the punitive approach, given that the punitive individual mandate was unpopular and removed, it is best to use a different approach to avoid this pitfall.
These are a few ways the administration could have done things differently, had former President Obama foreseen the roadblocks from his approach. The alternative design is not without flaws; it does not address all of the ACA’s issues, and new solutions often come with unforeseen problems. And in politics, there is no easy way to test the counterfactual when making quick, high-stakes decisions. Nonetheless, examining past decisions and thinking through how one could avoid past errors is how we, as engaged members of society, can improve upon decision-making in the future.
Policymaking is an iterative process, and the story of the ACA provides many lessons for our future leaders, whether one supports the policy or not.